

Should off-label drugs be allowed in the fight against COVID-19?
The bad news about COVID-19 continues to pour in. The “Delta variant” now makes up 98 percent of COVID cases in Washington, Dr. Alan Melnick of Clark County Public Health shared last Friday. Case rates now exceed levels in January, prior to mass inoculation by the three “EUA approved” vaccinations. “Delta is a game-changer,” he said.
“Israel’s Grim COVID Data Suggests Vaccines Alone Won’t Stop Pandemic” read one major news headline. They are perhaps the most vaccinated nation in the world. Yet vaccines designed when the original “alpha” variant was the only known type of COVID-19 don’t appear to solve the crisis as the number of “breakthrough” cases continue to rise.
Prescribing off-label or repurposed drugs is common. It accounts for 10 to 20 percent of all prescriptions written, although the practice is more common in specific patient populations like children and the elderly. “Physicians also might be more likely to prescribe off-label medications for patients facing life-threatening or terminal medical conditions for which there are limited or no FDA-approved alternatives,” states the AMA Journal of Ethics.
Clark County resident Nicole Wubben’s son is a lineman in Texas. Most of his work is outdoors. Yet he came in contact with a coworker who had COVID-19.
His entire family came down with the sickness COVID-19 triggers. In the midst of being treated for heat exhaustion, COVID hit him hard. The entire family was prescribed a regimen of drugs and vitamins which included ivermectin.
A week after receiving the drugs, her son is doing much better. His family is recovering too. They are all grateful for the medical care they received, and especially “the wonder drug” ivermectin.
Last month, the Food and Drug Administration (FDA) issued a press release warning people about the use of the antiparasitic drug ivermectin. News reports hyped people going to the hospital for taking the “horse medication.” In Mississippi two people were reported to end up in a hospital for wrongly taking the version of ivermectin meant for livestock. According to an Aug. 20 press release, that was not true. “No hospitalizations due to ivermectin toxicity have been directly reported to the Mississippi Poison Control Center or the Mississippi State Department of Health.”
Clark County Public Health dutifully followed Washington DOH guidance with the following.
“Ivermectin is an antiparasitic drug used commonly in humans and animals. Ivermectin tablets are approved by the FDA at very specific doses for some parasitic worms, and there are topical formulations for head lice and skin conditions like rosacea. But ivermectin is not an anti-viral (a drug for treating viruses).
“Evidence to-date shows ivermectin is ineffective against treating the COVID-19 and the side effects can be potentially dangerous. Using formulations intended for animals, which are often higher concentration, could lead to overdoses.”
Yet in Israel, an Aug. 2 news headline says “Double-blind study shows ivermectin reduces disease’s duration and infectiousness • FDA and WHO caution against its use.” In June, Oxford University began an in depth study of ivermectin. They reported that ivermectin is a broad spectrum antiparasitic that reduced SARS-CoV-2 replication in laboratory studies.
The U.S. media followed with a barrage of anti-ivermectin stories. “The Centers for Disease Control and Prevention (CDC) issued a new health advisory Thursday reiterating that ivermectin does not treat or prevent COVID-19. The drug, which is commonly used to treat parasites in humans and animals, is selling out at veterinary stores and has become a common prescription request across the U.S.”
Yet in 2019, the CDC advocated for the use of ivermectin treatment on immigrants. They advised the International Organization for Migration (IOM) physicians who screen the refugees for departure, and U.S. doctors who treat them upon arrival, to prescribe “all Middle Eastern, Asian, North African, Latin American, and Caribbean refugees” with ivermectin and albendazole.
Over the weekend, Rolling Stone magazine had to issue a “correction” about a false story published Friday, reporting hospitals in Oklahoma were being overrun with people who had taken the livestock version of ivermectin. “Oklahoma hospital system denies claim of gunshot victims left to wait as staff overwhelmed with horse dewormer overdoses” one local TV news station reported.
The story turns out to have been based on the claims of one doctor — claims that Rolling Stone and other media sources never checked.
The FDA approved the Pfizer-BioNTech vaccine, now named Comirnity for use in August. However, the FDA does not prohibit physicians from prescribing drugs off-label. Congress has repeatedly taken legal steps to prevent the FDA from interfering with the practice of medicine.
Yet protests continue to increase against Gov. Jay Inslee’s vaccine mandates. Seattle’s Jason Rantz shared “mass resistance arises as Washington makes it nearly impossible to get vaccine exemptions.”
Whom to believe
The politicians and heads of public health agencies have pledged to “follow the science.” Are they following the science when it comes to ivermectin and other off-label drugs? Whom should you believe?
According to many, the battle against ivermectin is because of federal restrictions contained in the Emergency Use Authorization (EUA) regulations. They prohibit new, not fully tested drugs from use if there are other “adequate, approved and available alternatives.” Big pharma would rather sell you $3,000 per dose remdesivir than $1-2 ivermectin, fluvoxamine, or hydroxychloroquine.
Daniel Horowitz said of ivermectin: “to suggest that it is not safe is a scandalous lie.” He went on: “precisely at the time when the shots are wearing off, the FDA not only quasi-approved the vaccine, but picked the leakiest of all to greenlight and also authorized emergency use of a third shot … of the same failed substance.”
The National Institutes of Health (NIH) currently says “both chloroquine and hydroxychloroquine increase the endosomal pH, which inhibits fusion between SARS-CoV-2 and the host cell membrane.” Yet the FDA revoked hydroxychloroquine EUA for COVID in June 2020.
Hatred of former President Donald Trump has kept researchers from looking into the antiparasitic drug ivermectin and other drugs to treat COVID-19, Kentucky Sen. Rand Paul told constituents last week.
“The hatred for Trump deranged these people so much that they’re unwilling to objectively study it,” Paul said to constituents in a Northern Kentucky suburb just south of Cincinnati. “So someone like me that’s in the middle of it, I can’t tell you because they will not study ivermectin. They will not study hydroxychloroquine without the taint of their hatred for Donald Trump.”
It’s also why they don’t research hydroxychloroquine, he said, an anti-malarial drug touted by Trump as a treatment.
An Ohio Judge ordered a hospital to treat a ventilated COVID-19 patient with ivermectin. Judge Gregory Howard ruled last week that West Chester Hospital, part of the University of Cincinnati’s health network must “immediately administer ivermectin” to patient Jeffrey Smith following his doctor’s prescription of 30 mg of ivermectin for 21 days, the Ohio Capital Journal reported.
In India and other poor countries, ivermectin has demonstrated amazing results. These include parts of Peru, Paraguay, Colombia, Argentina and Brazil; and in Panama, Namibia, Zimbabwe, Slovakia and Indonesia. Ivermectin reduced hospitalizations in Mexico City up to 76 percent, while a door-to-door campaign obliterated it in the state of Chiapas. These trends follow organized efforts to try ivermectin, are no coincidence.
Yet in the U.S. the barrage of bad press has triggered “ivermectin reluctance” on a level that rivals “vaccine reluctance,” creating horrible situations like this.
Facing intubation next, Tyrrell had had enough. “I’m terminal, if you unplug that [oxygen] machine, I’m going to die,” he told a doctor. “I asked him, after he’d already given me everything else, if I could take ivermectin.”
“You might as well drink bleach,” the doctor responded.
Stephen Tyrrell is alive today because he got ivermectin. “It saved my life,” he said. The 51-year-old Florida man spent 104 days in two hospitals and in rehab facilities. For his first 38 days in the hospital, his insurance company paid $385,000.
In anatomy of a failed policy, multiple success stories are laid side by side with awful tales such as mentioned above. Doctors are pressured by healthcare systems and government regulators, who in turn are pressured by politicians and their corporate sponsors.
Rather than support actual outpatient care, this is what we get from alleged protectors of U.S. public health, including the Food and Drug Administration, National Institutes of Health, and Centers for Disease Control, states Mary Beth Pfeiffer.
- Willful ignorance of the science supporting ivermectin – or any early treatment for that matter.
- Demonization of this safe FDA-approved drug, used on 250 million people annually, as fit only for animals.
- Speedy acceptance of drugs like woefully ineffective remdesivir in a system rife with conflicts of interest.
- A fantastical supposition that there is one way out of COVID: Vaccines.
- Greatly enriched pharmaceutical companies thanks to taxpayer largesse and something called the Emergency Use Authorization.
That statute in U.S. law allowed millions to be inoculated with a hot-off-the-presses, unapproved vaccine, as long as one explicit caveat was met: “there are no adequate, approved, and available alternatives.”
Of course, we know there were alternatives all along. Drugs to treat COVID have been sacrificed to vaccines.
CLICK TO PLAY VIDEO. Dr. Pierre Kory of the Front-Line COVID-19 Critical Care Alliance addresses a Senate committee and answers questions about the use and effectiveness of ivermectin.
In Israel, a recent news headline reports “$15 drug gets COVID patients off oxygen support in under week – study.” Fenofibrate is an FDA-approved oral medication. The results were published on Researchsquare.com and are currently under peer review. The UK study showed the drug reduced COVID infection by up to 70 percent.
Other existing drugs might have relegated COVID to a manageable outpatient disease by the first half of 2021. There are promising generics: ivermectin primarily but also fluvoxamine, hydroxychloroquine, budesonide and protocols that employ them with zinc, Vitamin D and more, reported Pfeiffer.
The news and potential benefits of these alternatives have been suppressed around the globe. “Countries – mainly, but not all, in the first world — have caved under pressure to conform to the U.S.-hatched strategy of expensive vaccines paid for by the government,” she says. Big pharma approves.
Dr. Pierre Kory broke the news in the U.S. last December, but has been vilified in the media. Nonetheless, he and his team continue their efforts to explore “repurposed drugs” via the Frontline Covid Critical Care Alliance (FLCCC).
In spite of suppression by major media outlets, the efforts of Dr. Kory, Dr. Paul Marik, Dr.G. Umberto Meduri, Dr. Joseph Varon, Dr. Jose Iglesias and their team of physicians is getting shared.
On Aug. 19, Matt Walsh shared an extensive story on ivermectin with his newspaper empire of 425,000, in a piece titled The battle for ivermectin. He introduces them to Michael Capuzzo.
Capuzzo is a former reporter for The Philadelphia Inquirer and The Miami Herald and the author of the New York Times bestsellers Close to Shore and The Murder Room. He is cofounder and editor of Mountain Home magazine.
Capuzzon has produced the single most complete story on the battle over ivermectin — a 10,000 word tome that truly tells as many sides of the story as is possible. Written in May, “The drug that cracked covid” is an amazing tale, a “must read” for people wanting to more fully understand what is happening.
He shared the following last week in an article titled: Believe It: A Top Old School Journalist Stands Up for Ivermectin and Free Speech.
“What’s so frightening about little ivermectin that The New York Times must daily drive stakes through its heart? And start again the next day with the garlic and the spike and hammer because the little pill keeps jumping from the casket, whispering it’s inconvenient, unstoppable truths?
“… A drug typically used to treat parasitic worms,” the Times lead paragraph states (except better known in human medicine as eradicating elephantiasis and river blindness in Africa in one of the great humanitarian achievements in medical history) “…that has repeatedly failed in clinical trials to help people infected with the coronavirus” (except in the 58 randomized and observational controlled trials of 10,200 people showing it strongly reduces transmission, time to recovery, hospitalization, and death). “The only functional strategy we have for getting control of COVID-19 is vaccination,” Dr. Irwin Redlener of Columbia University told the Times…(except in Mexico City, and many other places on Earth with brown and black and poor people the Times simply ignores, where the IMSSS Health Agency collapsed the pandemic with ivermectin, when 50,000 patients treated early with it compared to 70,000 not treated found a 75 percent reduction in need for hospitalization.) A show of hands, please: Is none of this news? Ivermectin propaganda is a whole new discipline, as robust as Victorian poetry or 20th Century fiction, and there’s no time to cover it all here.
“A counterbalance to the media slaying of ivermectin is Matt Walsh, owner of a group of award-winning newspapers and a fiercely ethical Old School journalist. He has had enough.”
Read more:
- Opinion: Why Bob Ferguson is wrong and what SMF is doing about it
 Silent Majority Foundation challenges Bob Ferguson over alleged rights violations in federal lawsuit.
Silent Majority Foundation challenges Bob Ferguson over alleged rights violations in federal lawsuit. - Silent Majority Foundation files lawsuit on behalf of former state employees who were terminated under policy requiring a COVID-19 vaccineSilent Majority Foundation files a lawsuit on behalf of former state employees alleging constitutional violations over a COVID-19 vaccine mandate.
- Letter: New movie on COVID vaccine victims deserves a watchRichard Beamish discusses the documentary on COVID vaccine victims, urging viewers to watch.
- Vancouver screening scheduled of ‘Vaxxed III: Authorized to Kill’Vancouver screening of ‘Vaxxed III: Authorized to Kill’ scheduled for Sept. 18 at Vancouver Mall 23.
- Study: Risk for getting COVID rises with each shot
 A new report from the Epoch Times warns that the more COVID shots an individual has taken, the higher the risk of getting COVID.
A new report from the Epoch Times warns that the more COVID shots an individual has taken, the higher the risk of getting COVID.





It is amazing how many liberals will just listen blindly to whatever CNN or NPR delivers to their listeners. These Rachel Maddow sycophants will oppose anything that closely resembles support for the other side, even when the recommendations are saving lives. I would suggest those who know better to preemptively get a prescription for Ivermectin now just in case you need it asap. Don’t listen to MSM they have been lying to everyone for the last two years. Do your own research and get the facts.
You forgot to add FOX to your sources. I agree with doing the research for yourself. This article is not research. So far clinical trials have been conducted on about 3,000 people with mixed results. Many of the studies that show positive results are preprints. They have not been published, and many probably never will be. This is not uncommon. One of the oft-quoted studies from Egypt involving about 300 people that purported to show positive results was recently retracted due to “plagiarism” and “data manipulation”. Perhaps studies conducted over the next several months will show ivermectin, to be the wonder drug that “conservatives” are looking for. In the meantime, 2.1 billion doses of several different vaccines have been administered world-idea with very few side effects. And highly positive results. In review of the the CDC adverse effects data, I see that the reporting of adverse effects are very low … about in a 1,000. I don’t understand why a vaccine developed under President Trump’s administration is not accepted by the conservatives. 94% of all America. Physicians are fully vaccinated as is President Trump and many persons in his former administration. For myself, a healthy 63 year old male, I went with the vaccination. For me the primary research I have done by reviewing the clinical trials for the vaccines, and ivermectin are a no-brainer. For those who choose to go the ivermectin route, I wish you all the best. For 99 out of 100 people either choice will not make a difference. The odds are in our favor. For the 1:100 where the treatment may make a difference, the choice could be a matter of life or death. I read every day about people who waited too long to make this decision.
Sir have you seen the numbers on VAERS on the CDC website that show the number of deaths and injuries from the vaccine? And Harvard estimates that this is only about 1% of the actual incidents that have occurred.
Pres Trump, while trying to fast track the vaccine, never said that this was the only way to fight Covid…remember when they distorted his words to make it seem like he was saying to drink bleach, well they have found that a certain kind of iodine is beneficial to ingest in the right amount and has prevented many from going into the hospital. Remember how he said we should try HCQ and was shot down by the media and Fauci? He was looking for other ways to treat covid and was not exclusively pushing the vaccine.
I don’t think he ever thought that shutting down the economy was a good thing and if it were up to him, he would not have done that. This so-called pandemic was treatable were it not for political interference.
This is an endemic, so we all have to learn how to live with it…just like the weather, colds, car crashes, etc.
I agree 100%
This didn’t age well, did it. Vaccines have not delivered the efficacy expected. Ivermectin has now been studied and USED ubiquitously with astounding results of survival from those who were circling the drain.
Why must you Politicize the drug like our fake leaders are doing? ‘MAYBE THE DRUG WILL BE THE WONDER DRUGS “CONSERVATIVES” WANT IT TO BE? WTF IS THAT??? ONLY CONSERVATIVES WANT SOMETHING OTHER THAN CONSTANT LIES ABOUT THE SUPPOSED “VACCINE” THEY TOOK THAT WAS SOLD TO THEM UNDER THE PREMISE OF SAVING THE COUNTRY, AS YOU COULD NOT GET INFECTED OR TRANSMIT THE VIRUS!!!! CAN WE ALL AGREE NOW THAT WAS TOTAL BULLSHT SINCE THE WHOLE VAXXED POPULATION NOW HAS OMICRON? DUH! FAUCHHI AND WERENSKI SCOOTED RIGHT AROUND THE 16-3 VERDICT BY THE CDC PANEL OF DRS NOT TO MASS INOCULATE THE ENTIRE PUBLIC WITH A BOOSTER JUST AS FAUCHI WENT AROUND THE PRDER BY PRESIDENT OBAMA NOT TO FUND GAIN OF FUNCTION RESEARCH! ENOUGH IS ENOUGH!
BRAINWASHED OR JUST IGNORANT OF THE FACTS, FOR 2 YEARS YOU HAVE BELIEVED IN A VACCINE WITH ABOUT 4 MONTHS OF TRIALS. NONE ON CHILDREN BUT YOU SOMEHOW KNOW FOR A FACT THERE IS NOT A SINGLE THERAPEUTIC THAT FIGHTS THE SARS VIRUS??? FUNNY LOOK AT THE New England MEDICAL JOURNAL IN 2020 WHERE DR FAUCHI HIMSELF WRITES , “Hydroxychloroquin has been found to an effective treatment for the SARS virus, especially when given early in treatment”! So what changed? EASY… Fauchi now sits on the board of directors of Modern and Pfizer and is also on the patents signed in 2015 and 2018 for the invention of a MRNA Coronavirus vaccine!!!! wake up everyone and smell the coffee,,,, THIS IS ALL SMOKE AND MIRRORS! The biggest medical lie in the history of the world! PERIOD! how much more proof do you need? This is
about power top control masses of people… 3 shots don’t wok so lets give you a 4th,.,,, just be quiet and do as your told! UH NO!
Point made: do your own research! However make it FACT based… from credible organizations that have the history in a reliability of accurate studies and research.
you referenced NPR as being biased and feeding listeners false information.
can you share any lawsuits brought against NPR about information shared on their broadcast ? doubtful !!
Credible organizations? And you will believe them cause they provide a piece of paper and claim it as facts just cause of your belief in them? Quit deceiving people.
Have you not dug around about why covid is all over the world and not in a particular country or a suburb or why it was released?
The current Russia and Ukraine war, why is Russia currently demonized and its people peasant citizens censored at the moment, while US and NATO/EU are portrayed like angels and that their righteous? Who is the cash cow in NATO and gives em power?
Who is the one that instigated and killed more innocent in wars if not around 70-80% by the honest and false sense of free, USA.
Afghan war of 2k 9/11 so called bin Laden attack, what about hanging of Saddam and the REAL reasons behind all this, including purpose release of covid by the US? Answer me honestly based on truth and not some paper bought out by the highest agenda bidder.
I can provide massive amounts for sealed classified documents that non of you will ever see, but why throw truth towards dogs that all they do is bark back and are conditioned to be a herd.
Just cause research was done or there is some kind of human made paper posted as proof doesn’t mean it is truth. Those that seek the truth will find it.
ahgGLDMU-BBS_W.L.#V_4_V
Hi John. Just a few thoughts. This is the sentence that really stands out for me the most. …”Using formulations intended for animals, which are often higher concentration, could lead to overdoses.”
I personally don’t mind if people want or don’t want to use invermectin. It’s up to them. Politics doesn’t come into it for me. I’d just like for them to use it, if they decide to, at safe dosages, and it would be good if they left enough available for veterinarians and farmers so that they can get it for the animals that are needing it for the parasites.
Jan —
You’re right. However the “problem” is that the media and the government isn’t telling people “use it in the proper doses”. They’re telling people “don’t use it” or “it’s not approved for COVID-19”.
Healthcare professionals are being threatened if they prescribe it for their patients. They could lose their medical license and their ability to care for their patients.
That’s the real problem.
Nobody that I know of, is telling people to get their hands on ivermectin WITHOUT first consulting a doctor, and without getting a prescription.
Thanks for reading the article!
IT is disgusting. I have a medical friend who prescribes this but was told last week he has to stop or loose his license. The week before he prescribed this antibiotic for a friend. It worked.
and many pharmacies will not even dispense it anymore. So sad
Sad, but true.
There’s lots of information online on how to mark and properly dispense veterinary-grade Ivermectin when medical grade is unavailable. This webpage has a table with dosage/kg advice-
https://www.americanpartisan.org/wp-content/uploads/2021/08/index.png
I’m fine suggesting people talk to their doctor about this, but I cant condone self-diagnosis and self-administration. Please dont be an enabler.
Thanks. The problem already exists. There are black markets in many countries. where governments are being told not to use it. I would just like to have a safe supply. Regardless of its benifits. We already know it is very safe and should be made available at very low cost for people in less developed countries that lack vaccines and good medical services. We do not have many options for early intervention. Most people are just isolated until they get sick. I know of numerous doctors that use this as an early intervention treatment. It is not an anti-viral drug. It is being used to reduce inflammation. Especially in the lungs. Preventing a cytokinin storm. And maybe blocking the virus from entering cells with the ACE 2 proteins.
and what if your doctor refuses to give you what you ask for because he listens to the CDC and NIH, like my doctor. I had to go elsewhere.
Thank you
Can you please give us the link to find this on the internet?
That would be helpful. Many thanks,
Excellent – Thank you!
Thanks for this excellent and important article John. I was saved by ivermectin, dexamethazone, azythromycin, and many supplements, provided by a brave doctor who is risking his medical career and pouring out his life to save others. My husband Danny, the love of Christ, and these medicines, especially ivermectin, saved me. It wasn’t easy to get. Thanks for getting the word out. The people who are suppressing these treatments are EVIL and should be in jail. Blessings to you John.
P.s. my life matters too.
Thank you for writing such an informative and well-researched article!
It’s neither well researched or informative. He has the wrong data for India, he quoted his own paper about death rates in Argentina and Mexico – which were wrong….he quoted the FLCCC who made two studies central to their argument – both of which were withdrawn for fraud.
Jim — here is the official follow up on one of those studies you note was “withdrawn”. It was withdrawn without consulting the author.
The end result was that even if you removed the one bit of data being questioned from his study, the net results overall was that ivermectin still provided substantial benefits.
https://covid19criticalcare.com/wp-content/uploads/2021/09/Response-to-Elgazzar.pdf
Yes. The professional metaresearch projects made clear allowance for the unreliability of the information. If you look for information from Dr. Tess Lawrie she explains the process. Many more studies were also used. A number of studies have been done with the below-recomended use. Making Ivermectin look inneffective. False studies by the drug industry. Using Ivermectin solely for critical care is bound to be ineffective for many people that are already seriously ill. Ivermectin is best used for protection or early intervention. Acting to stop the destructive cytokinin storm before people become seriously ill. COVID is a very complex disease. Most treatments for COVID are not antiviral drugs. And many have multiple uses. That is why repurposing drugs for COVID 19 was so important. That is what brought attention to Ivermectin. Thousands of known and safe drugs were tested in labs to find potential treatments. Ivermectin is not a miracle drug. It should be used with a combination of other treatments. The FLCCC doctors alliance website has suggested protocols.
Jim. A well conducted senate sub committee hearing investigated and dispelled virtually everything you obviously just fabricated for what ever your reason might be. You would be well served if you would really look into the 10’s of thousands of lives still living because of Ivermectin before making a pure fool of your self and misleading others along the way. Some of these are my own family members that were told they could be made comfortable as they were dying and our Dr. (with legal help) literally forced some nurse assistants out of the way to administer the Ivermectin. After an extended period of rehab for my dad, all survived and are doing well. This Houston Dr. has now saved 100″s of lives that you would have rather sent to the grave to prove your point. Shame & double shame on you.
The statement that two individuals in Mississippi were hospitalized due to Ivermectin use is not true. It is false information spread by repeating what’s been reported elsewhere. If you check the Mississippi Public Health web site their official statement on August 20th (the same date as the cited news report), available at https://msdh.ms.gov/msdhsite/_static/resources/15400.pdf says “No hospitalizations due to ivermectin toxicity have been directly reported to the Mississippi Poison Control Center or the Mississippi State Department of Health”. The statement makes clear that they have only fielded phone calls from people concerned about potential overdoses. As an aside, it is extremely difficult to overdose on Ivermectin. People have been given 10x the recommended dose with no detectable side effects.
Otherwise a well written article.
Thank you! Trying to track down every single nuance is tough. I appreciate this added information and will include it in the article.
Thank you SO MUCH for this excellent article! Pointing out the facts, in the face of all these lies. It truly helps, since nearly all the “trusted mainstream media” seem to be attacking anything outside of the CDC -FDA pronouncements.
I used to have a habit of going to CNN for “news” but was sickened by one of their videos recently; the one claiming Joe Rogan had taken “Horse De-Wormer” and claiming that “Ten studies showed Ivermection does not work.” I can’t stomach CNN any more. (Not that I’ll go to Fox either.) Your article is a rare find!!!
The most unbiased source of information about what’s going on I’ve found is peakprosperity.com
Seriously? Check this out:
https://www.motherjones.com/politics/2020/02/coronavirus-youtube-creators/
QUESTION EVERYTHING!
John,
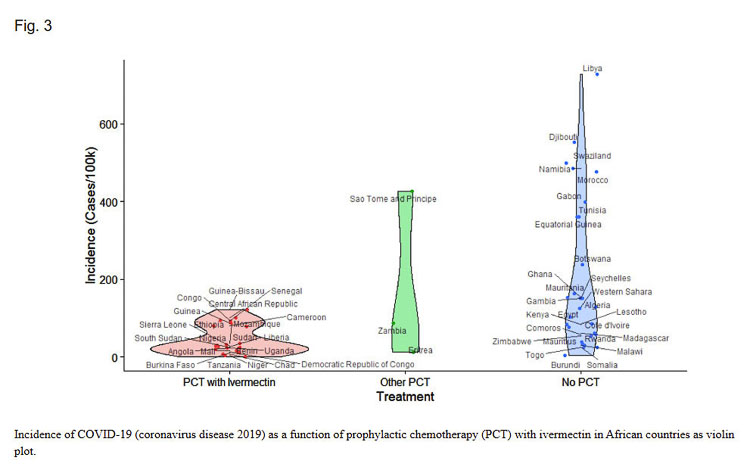
Although I have been to date skeptical of Ivermectin as therapeutic for COVID, I still try to keep an open mind. I reviewed the NIH report containing the violin chart that you provided in your article. I noticed that the NIH report only contained data through October 20, 2020… This is really only about 6 or 7 months of data. So, I decided to load up the most current data from the same source used by the NIH report. This included about 11 more months of data that was not in the original report. I focused on the first group I will call Group A (countries using Ivermectin) and the third group (countries not using Ivermectin), which I will call Group B. There were a total of 22 countries and 850,000,000 inhabits in Group A and 28 countries and 460,000,000 people in. The bottom line is there 4.7X more COVID cases reported in Group B then in Group A. 7,945 cases per million in habitants in Group B vs. 1,677 cases per million inhabitant in Group B. Furthermore I found a similar but larger ratio for total reported COVID deaths in the two groups. There were 6.2X more COVID deaths in the countries not using ivermectin. I found 194 deaths per million inhabitants in Group B compared to 31 deaths per million in Group A. In summary this additional data further strengthens the authors original thesis, that Ivermectin might be an alternative therapy to being vaccinated.
So, I am one skeptic who is somewhat less skeptical now then when I initially read your article. I for one try to keep an open mind, and only ask all of us do the same. I may have my biases, but I am influenced by what the data indicates. We all really want the same thing… We want to come out the other side of the pandemic and be happy and healthy.
Thanks for an interesting article, and especially the chart.
R. Sisson —
THANK YOU so much for doing the added research, and providing it here.
“If” you are inclined, we would welcome a “letter to the editor” or column, where you submit your research so that our readers can consider them as they try to decide how best to respond to the current, growing numbers of the “Delta variant” cases.
I really hope no one listens to you. You are spreading medical disinformation and we are adding you to the Medical Disnformers Facebook page. Pierre Kory quoted TWO studies that were retracted. He is known as a kook by two of his former employers. The Argentina study he quoted to congress was laughably bad and it’s shocking he quoted it. https://www.nature.com/articles/d41586-021-02081-w
The India data you cited is not even close to true
https://www.poynter.org/fact-checking/2021/theres-no-proof-that-hydroxychloroquine-or-ivermectin-caused-a-drop-in-cases-in-india/
There are no – NONE – CRT studies that show Ivermectin work in fact most studies show the opposite https://www.medrxiv.org/content/10.1101/2021.05.21.21257595v1.full.pdf
Did you even bother mentioning that doctors from the FLCCC have said that hydroxychloroquine does not work? And that at least two of their doctors have advised people to get vaccinated?
Of course you didn’t. Because you have no morals.
https://medicalupdateonline.com/2021/05/choosing-and-using-ivermectin-for-covid-19-in-india/
Thanks for the information. Too bad, you cannot fix stupid, and demo-lemmings are the stupidest.
The FLCCC includes links to studies and analysis for residents to research for themselves. Most of the media outlets are heavily funded with Big Pharma advertising dollars and promote Big Pharma solutions, censoring information about the side effects of experimental products. Ivermectin isn’t producing $BILLIONS for Pharmaceutical companies and those who invest in them like Gates has. There is no one size fits all practice of medicine, and the role of government is not to prescribe treatments for all residents, especially experimental treatments with risks of serious adverse events after vaccination, including death. I hope and pray WA residents will be able to maintain the right to make their own medical choices, with the input of healthcare providers that a person chooses.
So, you see why people are skeptical, right? It beginning to look like when the media and govt types all have the same hymnal and adamantly declare something you should or shouldn’t do, it is NOT in your favor. Then they call people a conspiracy theorist. I am thankful for this article and courage it takes that is seemingly becoming required. speaking of which, there is now word of some in Washington moving to forbid the FDA from interfering with the practice of medicine ( keeping us from Hydroxychloroquine)
What could drive people to do these things? Looks like an agenda to me, but for what? Money? Population control? (proteins that don’t go away)
Fear tactics…then lockdowns…then pressure tactics…then outright taking action to strip you of your job, (no money, no house, food, family, education etc.)- gangster tactics…what could be next?
A common problem seems to be how, why and when Ivermectin should be used. This is a reason why many studies do not show good results. And why thousands of doctors support its use.
COVID 19 is not a simple viral infection. COVID disease harms people in many ways. And the COVID virus itself does not do significant damage. COVID is a viral, autoimmune, cardiovascular and pulmonary disease. And there are many different treatments for COVID disease that are not antiviral drugs. Warfarin is being used in some countries to treat COVID. Warfarin is not an antiviral drug. Warfarin is very toxic. Much more than Ivermectin. But why do they let doctors use such a dangerous drug as Warfarin? Warfarin is also used for animals. But not to make them better. We now have other drugs that can replace Warfarin in developed nations. Warfarin also can interact badly with many other medications. So why is the WHO not condemning Warfarin? A well-known toxin, used to kill animals, does not kill the virus and can be used for, more than one use. Warfarin can interact with Ivermectin. So Ivermectin should be prescribed by doctors who understand the potential interactions.
Most of the drugs used to treat COVID disease are not antiviral drugs. We have few effective and cheap anti-viral drugs. That is why we use vaccines instead of antiviral drugs.
Ivermectin is not an antiviral drug for humans. It does not kill the virus. But Ivermectin has other actions that may help to treat people with COVID. One action is blocking the movement of the virus in and out of human cells and the cell nucleus. This can effectively stop viral replication. And Ivermectin may also have very strong anti-inflammatory effects.
Ivermectin has been in very safe human use for 40 years. Billions of people have been treated with Ivermectin. Ivermectin protects millions of Africans each year from disabilities including river blindness. Millions of children have been saved from deadly viral diseases in less developed nations where they do not have reliable supplies of clean water.
Many tests have shown Ivermectin to be both effective and ineffective.
A major problem seems to be how Ivermectin is used. If it is being used for people that are already very ill then the chances of success are lower. Ivermectin is best used for prevention and early intervention before people become seriously ill. Before the human immune system produces a toxic cytokinin storm in the body. The cytokinin storm triggers a potentially deadly autoimmune response
Doctors currently have no effective early response treatment. Most people are told to stay at home and isolate until they recover or need critical care in a hospital.
Ivermectin may be a very effective option for people that are at risk, Have recently been exposed to the virus, or they have symptoms of COVID.
The FLCCC developed the treatment for acute care in hospitals where people are already very sick and can not breathe effectively. This has become a standard treatment worldwide. This is only to be used when people are seriously ill with lung congestion. The most deadly stage of COVID.
The FLCCC protocol for Ivermectin is that it can be used for prevention, early intervention, critical care and post COVID long haulers. The FLCCC website has collected research from around the world to develop their treatment protocols.
Treating people who are already critically ill is not like to produce very effective results. Even the use of steroids which has been very successful does not save everyone.
Why should billions of people in less developed nations not have this treatment option when they do not have access to vaccines or effective medical care.? Why is it so dangerous that they can not use Ivermectin for COVID but it is safe for parasites?
Doctors should have the option of using Ivermectin and people should be able to get a safe supply from their chemist.
Currently, Ivermectin is mostly being supplied in the black market where doctors have no control and the product may be of very low quality.
Allowing Ivermectin as a medical treatment for COVID will reduce the risks.to people’s health. It is very safe and cheap.
Why is the medical industry, the drug industry and WHO using so much of its influence and resources against Ivermectin?
Why is the WHO blocking the publication of Ivermectin research?
Why is the media being blocked from fairly reporting of Ivermectin?
Is Ivermectin a threat to new drugs that are in development? Drugs that are very similar to Ivermectin.
There is something very wrong with this issue.
The FLCCC website, https://flccc.net includes interviews with doctors who have treated patients, prevention/ immunity building info, studies, and more.Home interventions like certain mouthwash gargles (eg,Listerine antiseptic mouthwash) and certain nasal sprays are reported to have been effective for many.
When people make misatakes during a crisis, they call that the fog of war…in this case those in power have created the fog machine of war.
As of August 27, 2021 our local Public Health Department began an active campaign to suppress Ivermectin by using pharmacists to report any physician who prescribes Ivermectin for covid.
Read it yourself:
https://clark.wa.gov/media/document/103481
“Pharmacists receiving prescriptions for ivermectin for the treatment of prevention of COVID-19 should use their professional judgement in determining whether to fill them. If you have concerns related to the prescribing practices of a practitioner, it may be appropriate to reach out to the corresponding licensing board or commission. “
That’s what happened to friend of mine who prescribed it for a mutual friend. I went to pick it up for her at her regular pharmasee (Wal-mart). They refused to fill it, so then she tried another.(won’t say who because I don’t want the murderers to bully them). She finally got it and did much better. However, I think the wal-mart pharmacist turned the doctor in & he and his partner have been told they will loose their license if they prescribe it again.
Why are these doctors being punished for prescribing invermectin. We use all kind of drug on label and off label to treat. The results are in And the results say it works who is behind advocating not to use this drug. Big pharm ? Whoever it is,. They should be held accountable for there actions.They are costing people there life’s.
Hmm? Ivermectin is for parasites and it DOES work for this corona. This corona was developed via gain of function from a mammal (bat). Could it it be that an animal parasite is part of corona? For a reminder, humans are mammals also. Animals and people have long taken to some degree the same vitamins and medicines.
What?
“Laboratory testing of ivermectin” means just that…it was not studied in humans, but in a lab. The data shows that ivermectin can reduce replication of the virus, but at the dosage necessary would cause toxic in humans. It’s not “liberals” who believe the CDC, it’s people who know how to read studies and would rather take two shots than worry about getting sick and taking something THAT IS NOT PROVEN TO CURE OR TREAT COVID.
Aaron:
You are correct that laboratory testing is different than testing on humans for Covid.
That being said, ivermectin HAS been tested on humans. It may be one of the most “tested” drugs in modern history. It is completely “safe” for humans to use, when prescribed by a trained medical professional.
It is estimated that between 10 and 20 percent of all medications are prescribed “off label” — not for their FDA-approved uses. The FDA, NIH, and the entire medical establishment allow healthcare practitioners to “try” just about anything to save people’s lives and improve on their health.
Ivermectin appears to be working in certain states in India. It appears to be working in certain states in Mexico and Latin American countries.
We simply want people to know and make informed input to their healthcare providers. Given that we are experiencing another “wave” of Covid-19 triggered by the Delta variant, and that perhaps 25 percent of individuals getting it are “break through” cases, there is nothing wrong with these people and their healthcare providers discussing alternative medications and therapies to improve care and outcomes.
It has been used in humans as an anti parasitic. For anyone who has taken ivermectin and recovered from covid, the outcome is almost certainly coincidental. It’s so interesting how people will avoid a proven vaccine and instead choose a completely unproven drug to treat the illness that vaccine would prevent.
fyi, I work in critical care and I can assure you that the Pfizer and moderna vaccines work. I had a visitor ask if their loved one could get ivermectin and I had to explain to them what I just said. They thought that the government was conspiring against them and were hell bent on trying every experimental treatment there is, but would not get vaccinated because they “don’t believe the government”…the stupidity is tragic…
Aaron –
This is from the NIH.
https://www.covid19treatmentguidelines.nih.gov/tables/table-2e/
Aaron, could you please respond to “Margaret’s” post below? I’m neither advocating for or against. I’m just looking to get the general response of the “india study” from someone who believes Ivermectin is ineffective. Coincidence? False reporting?
Aaron…. did you just say “PROVEN VACCINE” have you been in a cave for the last month,, There are millions and millions of triple vaxed people now infected with Covid 19 yet again!!! That proves the vaccine is ineffective and the know it the whole time… the last thing they wanted was a drug that costs 12 cents and can’t be patented to be making people well! their MONOPOLY of illegally taking over the private health health choices would be gone as well as their gravy train of no nearly 1/4 trillion in profits from these fake vaccinations! I’s sure you do know that Fauchi has signed deals with Modern and Pfizer from 2015 and 18 for the rights patents and profits of all MRNA vaccines!!!! if you don’t know this… wow!
Widespread ivermectin use has caused a 97% drop in coronavirus cases in Delhi, India“Earlier in the year, India dealt with a devastating post-vaccine wave of the coronavirus. This post-vaccine outbreak affected the country differently. In states that did not use ivermectin, cases soared. But the data shows that by the end of May, this second wave of COVID-19 was under control in parts of the country that treated patients with ivermectin….
In Delhi, health authorities began treating patients with ivermectin on April 20. At the time, the metropolitan area of 30 million people was dealing with nearly 30,000 new cases daily.
By the end of May, COVID-19 cases in the metro area were down to less than 1,000 new cases per day. This is a 97 percent reduction in new COVID-19 cases in just five weeks.
The number of deaths per day also fell from nearly 300 in April to slightly above 100 by the end of May.
Similarly, momentous drops in COVID-19 cases could also be seen in at least four other Indian states that used ivermectin for its COVID-19 patients.”
Read this: https://medicalupdateonline.com/2021/05/choosing-and-using-ivermectin-for-covid-19-in-india/
what I need to know now is the name of a physician in the Vancouver /Portland area who is pro actively treating Covid patients as an out patient ,early treatment ,with Ivermectin and the I-MASK protocol. I do not have covid but I am looking for a new PCP that is open minded and smart enough to see that this medication works and will not back down to the fools who have made this political and the entities that are threatened by an off label generic drug due to big money interests . Right now ,I know more about Ivermectin and the mounds of small clinical trial results and real world clinical usage than my doctor knows . If he is going to have blind faith in the NIH , FDA ,CDC and WHO , then can I really trust him to treat me when I need him ? Anybody have any M.D. names in the area ?
Clark County People you can hold your heads high.
good article!
Now I only smile when anyone calls IVM a horse de-wormer or any other tale. I’m happy that they take the jabs.
Coming to an informed decision requires…..well, information.
How much information?
And from who ?
Some will say that the information we received from the CDC is reliable because they are professionals.
Ok, fair enough.
Could we assume that a district prosecutor is a ‘professional’ ?
If so, does that mean that the jury can come to an informed decision based on statements & testimony exclusively from the prosecution?
NO.
They would have to give the Defense a fair chance to also get a word in.
Just saying.
* If the FDA does approve Ivermectin for covid treatment, the mass tort ‘ambulance chasers’ will be at the ready, racing to assemble class action against Mrna manufacturers.
Why is it that with all the discussion, I have never seen the question of what role, if any, has Ivermectin in reducing vaccine side effects (I am being forced to get jab at work) I had covid 6 months ago. So vaccine efficacy is not important to me at this point. FLCCC had no info on this subject. Thank you for any info.
Some people are fighting for their jobs, and medical freedom. Learn about YOUR Rights: COVID-19 shots The adverse health events reported after COVID vaccination cannot be effectively treated in far too many cases. Deaths have also been reported after vaccination. WA state: 34 yr old :Male died after Pfizer vaccine.Forensic Pathologist after full autopsy determined patient was a healthy adult with no heart disease, no liver disease, and no pneumonia. Coroner determined after toxicology report that covid 19 vaccine was the only contributing factor. Everything else was ruled out.
Died June 25th after cardiac arrest on June 23rd, 8 days after his vaccine.VAERS ID:1578593See VAERS COVID Vaccine Data Show Surge in Reports of Serious Injuries See also Vaccine-Injured Speak Out, Feel Abandoned by Government Who Told Them COVID Shot Was Safe
Another website to review, https://thecovidblog.com
You neglected to mention that the CDC reccommended the 2 dose regimen of ivermectin for middle eastern immigrants. That is a treatment for parasites, not COVID. Didn’t fit your narrative ??
You can now add Japan to the list of countries who are using ivermectin with great success.
Invremectin saved my life from Covid. I was deathly sick by the fourth day when I took my first 5ml bottle of Quanox .06%Ivremctin. With in 24 hours my symptoms improved and after second dose and 48 hours later I was free of infection.
Go about 30 or 40 comments back up and read my personal experience. Thanks
If any of you have time to read my comment similar to Bill’s, please go back up about 25 or 30 replies. This stuff saved a big part of my family. Thanks
If you are close to the Houston area ,there is an Internal Medicine Specialist that is in private practice there in Houston that has saved 100s of lives by using Ivermectin as her primary starting Covid therapy. She is fighting to keep her license with the help of a large law firm in that area. What the authorities (LOL) are trying to do to her is what should be against the law. My son/his wife ,my granddaughter and her husband all came down super sick with this scourge. This Lady Dr. treated all of them. The kids (29 and 30) were up and running in about 72 hours and my son and daughter in law were done with it in just less than a week. My son is self employed. You could say she probably saved his life also or at least his lively hood.
I am a 72 year old man and relatively healthy. I’ve gotten all three shots of the Maderna vaccine, and am pro-vaccine. However, should I contract SARS Covid 19 I want the OPTION of procuring and taking ivermectin early on in the disease process, but it appears the this may not be possible in the politically charged environment we now live in here in the USA. I really dispose our governments interfering with the ability of doctors to prescribe whatever they fell is beneficial for their individual patients.
It was the case when this was published, and is the case now, that ICUs are occupied by 90+ % unvaccinated people.
I had 6 of my friends that took Ivermectin and Hydroxychloroquine a z-pack and perscription cough medicine and recovered from covid. I could not even get my doctors to try these drugs. Why? 50/50 chance. What happened to the term Practicing physicians? You try anything to save lives. My 68 year old husband passed away and the only thing the doctor asked me was why he did’t take the shot. When I told him he actually worked for 39 years for the largest IV solution plant in the WORLD and got extremely sick off of two vaccines in the past for a week both times his exact words were “But he didn’t die did he”? What a wonderful bedside manner. It was like “take the shot or you will die”. That’s what happened. There are medications out there to combat covid and I now have a doctor that will prescribe these for me in another state. I live in NC. Go figure! My doctor has saved over 12,000 covid stricken patients my last count and has only lost 2 to 3 patiens due to them NOT getting their meds in time. I have learned so so much too too late since losing the absolute love of my life. Please STOP being a democrat or republican….just be a good person…caring and compasionate reguardless. Life is so precious and we have not treated it as so. My husband’s doctor of 40 years now knows and he is very very saddened by what took place in his large clinic, or should I say what didn’t take place.